“It’s hard to even visualize the concept of one in a billion. It’s like having a billion one dollar bills and you have to find the one with a typo. All the dollar bills kind of look the same, so how do you sort through them and figure that out?”
Shannon Stott, PhD
Finding one in a billion is exactly what Shannon Stott, PhD, and Brian Nahed, MD, MSc, set out to do.
They have been working together at Mass General for a decade now, but come from completely different backgrounds; she is an engineer and he is a neurosurgeon.
Only at a place like Mass General, could these two work together to find a new way to diagnose and treat one of the most aggressive types of cancer: glioblastoma.
Where Engineering and Neuroscience Meet
After being introduced in the labs of Mehmet Toner, PhD, Dan Haber, MD, PhD, and Shyamala Maheswaran, PhD, Stott and Nahed began working methodically to identify various types of tumor cells in the blood.
After being inspired by the group’s success with other cancers, Nahed wanted to test for brain tumor cells circulating in the blood. No one else in the world had shown that brain tumor cells could even be found there.
Unlike other types of cancers, brain tumors generally do not metastasize or spread throughout the body, Nahed says. Most believed that these cells did not pass through the blood-brain barrier and into the bloodstream, and that if they did they would be next to impossible to identify.
That’s where Shannon Stott’s engineering background came in.
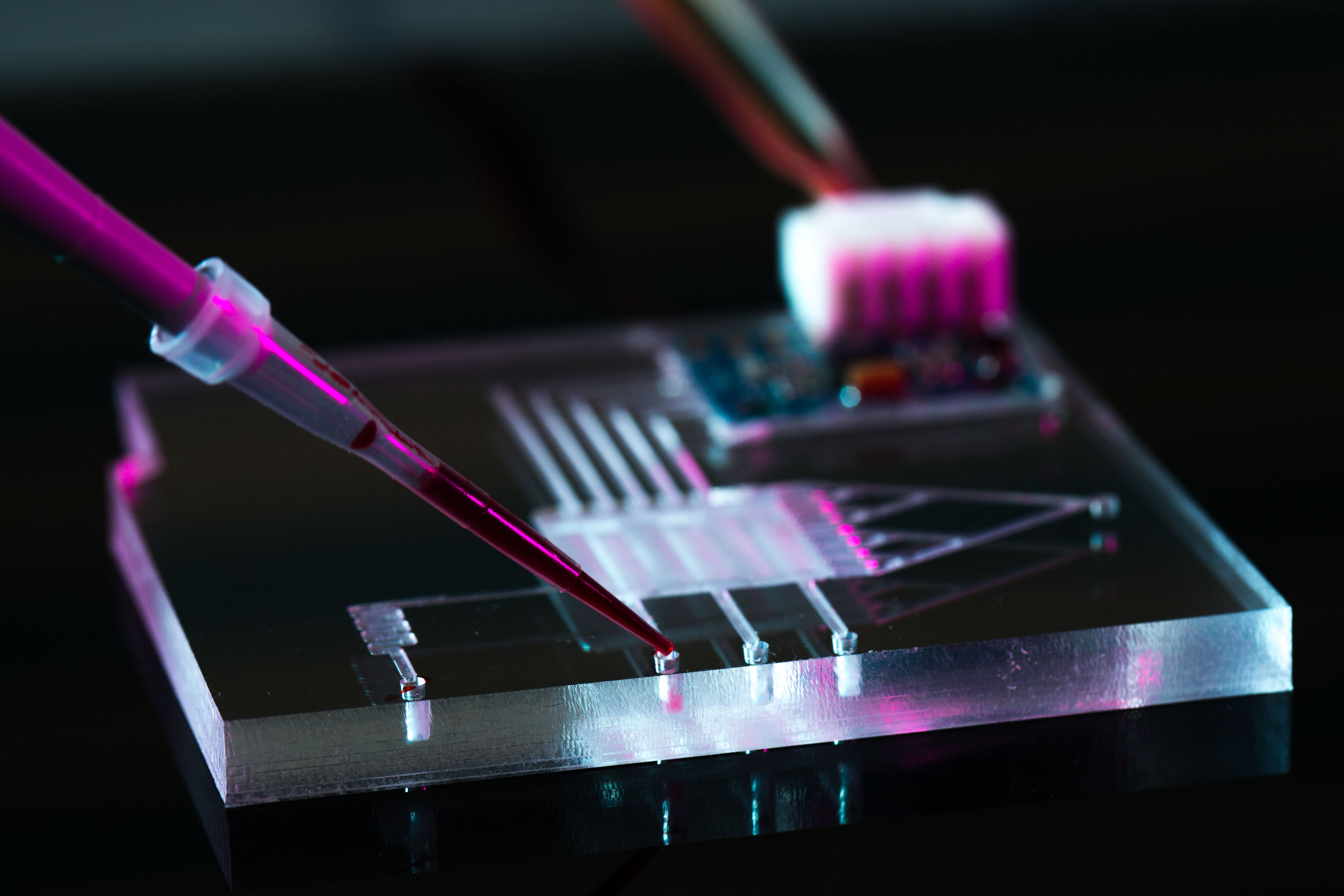
Using her backgrounds in microfluidics, particle movement and mechanical engineering, Shannon worked with a team of scientists and engineers to develop a device that could sort through the billions of cells in vial of blood.
Alongside Dr. Nahed and other researchers, they troubleshot to see what was the most logical and efficient way to identify the brain tumor cells. At first, they were targeting specific markers on the tumor cells, but they soon realized there was no perfect marker to target and decided to go for more of a process of elimination-approach.
“The tumor cells are like needles in a haystack. Initially, we assumed we knew what the needle looked like, and we tried to pull out the needles. Then, as we started to learn more, we realized we actually don’t know what the needles look like because it is hard to define them, particularly for brain tumors. But, we know what the hay looks like. We know what red blood cells look like, we know what platelets and white blood cells look like, so let’s get rid of those and see what’s left behind.”
Shannon Stott, PhD
After several bouts of trial and error, and working with a large team over a number of years, they created the first chip-based device capable of identifying and analyzing circulating brain tumor cells in 2016.
They are now able to evaluate blood samples at a highly rapid rate, with their device analyzing 30 million cells a second in a single-file progression. The blood is processed through a chip-based microfluidic device that can identify biomarkers, perform a drug screen, monitor a patient or create a summary of physiological mechanisms.
What’s next?
Now that Drs. Nahed and Stott have proven the brain tumor cells exist in the blood, they are looking to see what information they can gather from these cells.
One possibility is finding a way to monitor brain cancer in real time. If clinicians could diagnose, monitor and treat patients using information from these cells, it could have a profound effect on cancer treatment.
Right now, after a patient receives their initial brain cancer treatment, clinicians monitor their patients’ progress by simply evaluating their symptoms and looking at a scan.
If the scan is clear and the patient is not presenting with symptoms, the treatment could be going well. But sometimes a scan will show something that looks like the tumor has returned, when it in fact has not.
The phenomenon is called pseudoprogression, and it is an inflammatory response that can actually mean a patient is responding positively to treatment, Stott says.
This can create a difficult situation, because if a patient is responding positively to treatment, a clinician would not want to take them off their treatment course. But if the tumor has returned, a new course of action must be taken. The problem is there is no perfect way to tell the difference.
With their technology using blood samples, Stott and Nahed are hoping to one day monitor a patient’s treatment course and check for changes in the concentration of cancer markers or changes in the markers themselves.
Their technology could also help in the cases where tumors are inoperable.
If there is a tumor present in a child, or in a location that is dangerous to operate in, getting a diagnosis and coming up with a treatment can be very difficult, Nahed says. But if there were a way to identify the tumor non-invasively, it could be game-changing.
About the Mass General Research Institute
Research at Massachusetts General Hospital is interwoven through more than 30 different departments, centers and institutes. Our research includes fundamental, lab-based science; clinical trials to test new drugs, devices and diagnostic tools; and community and population-based research to improve health outcomes across populations and eliminate disparities in care.
Support our Research
Leave a Comment